The Ever-Changing Morphology of Calf Perforating Veins and How Your Practice May Be Affected
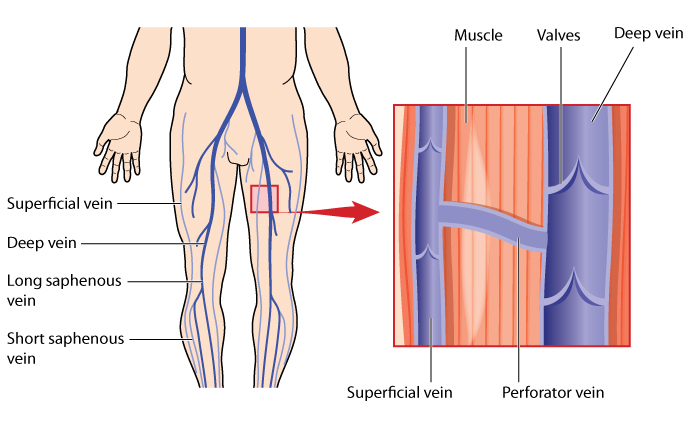
/Perforating veins are small veins which allow blood to transfer from superficial veins to the deeps veins. These veins are capable of refluxing similarly to the truncal veins, and may contribute a large part to varicose veins, trophic changes, and venous ulcers if left untreated.
Attached to this post is a great read on the ever-changing morphology and hemodynamics of calf perforator veins post-EVA, stressing the importance of reevaluation during post-ablation follow-up exams. Often we see patients come in for continued vein treatments from previous locations, only to show more signs of increased swelling and venous hypertension than when they began the treatment process. Before every procedure, it is crucial to evaluate the nature of the pathology that the patient is scheduled to treat that day in the event that the vein was not reevaluated during the follow-up exam. A situation which seems to occur quite often is that a perforating vein is previously documented as incompetent in the original reflux report, but is no longer incompetent due to the offloading triggered by previous saphenous ablations and is subject to treatment anyway. This leads to increased venous hypertension and undesirable results. Not only are previously incompetent perforating veins now potentially competent, but neovascularization may have occurred in the lateral aspect of the legs due to venous flow redirection, and new perforators are subsequently left uninvestigated.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4557325/#!po=85.8696